


- Biology and Evolution
- Science
- Science and Technology
- Scientific Discoveries
- Technology and Innovation
Historic Breakthrough: China’s Brain-Computer Interface Leaves Neuralink Behind
Medical accuracy note: The clinical information in this article has been verified against publicly available regulatory filings from China’s NMPA and NHSA, the medRxiv clinical preprint (October 2025), and reporting from MIT Technology Review, Scientific American, Nature, Bloomberg, and Reuters. It does not constitute medical advice. Readers with health concerns should consult a qualified physician.
A paralyzed man named Dong Hui raised a cup to his lips and drank from it. He had not been able to do that independently for more than a decade.
The device that made it possible became on March 13, 2026, the first invasive brain computer interface to receive commercial regulatory approval anywhere on Earth. China reached this milestone before Neuralink, before any American company, and before any European regulator had come close. That approval matters because a brain-computer interface has now crossed the line from laboratory demonstration to something a physician can actually prescribe.
What You Need to Know: 6 Key Facts
- Approval date: March 13, 2026, China’s National Medical Products Administration (NMPA), confirmed by Xinhua, MIT Technology Review, Scientific American, and Bloomberg
- Device: NEO (formally NEO-ONE SCI), a wireless epidural implant by Neuracle Medical Technology and Tsinghua University, Shanghai
- What it does: Reads motor-intention signals from the brain’s outer membrane and transmits them to a pneumatic rehabilitation glove, restoring hand grasp in patients with spinal cord injury
- Who qualifies: Adults aged 18 to 60 with C2 to C6 cervical spinal cord injuries who retain some upper arm movement but cannot fully grasp
- Insurance timeline: Within 12 days of NMPA approval, China’s National Healthcare Security Administration assigned NEO a medical insurance code and completed procurement listing, a sequence observers called “light-speed coding” (Hello China Tech, June 2026). However, the full device cost is not yet reimbursable through standard government channels
- Neuralink’s status: FDA investigational authorization only as of mid-2026; Bloomberg-cited investor documents project commercial approval around 2029 at the earliest
Brain-computer interfaces are growing rapidly as the technology moves toward commercial use.
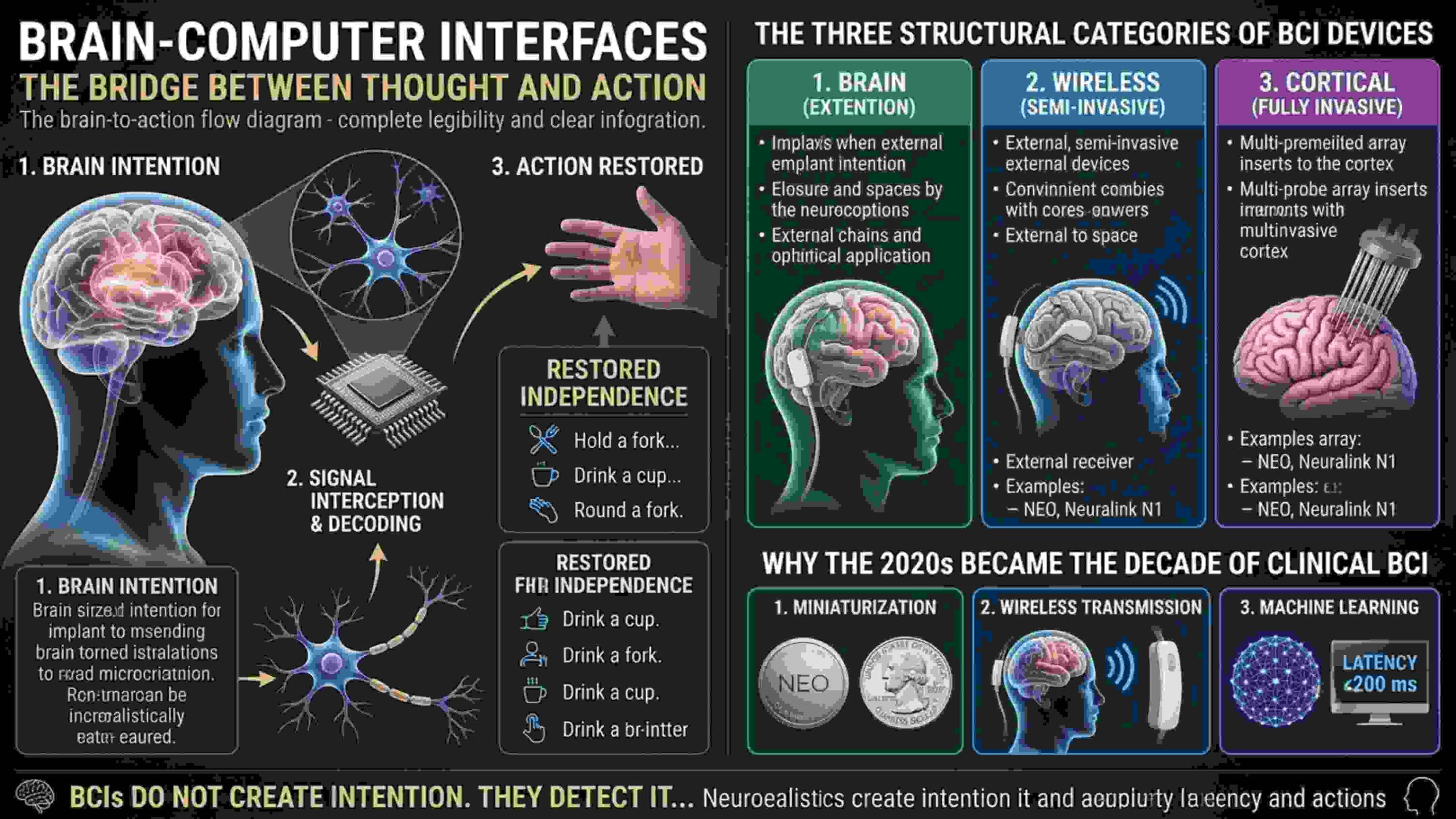
Every time you decide to pick up a glass, populations of neurons fire in coordinated sequences across your motor cortex. Those signals travel down your spinal cord and tell your hand muscles to contract. For a person with a cervical spinal cord injury, that signal never arrives. The brain sends it. The hand never receives it.
 Technology and Structural Categories png")
A brain computer interface intercepts the signal before it reaches the damaged spinal cord, decodes the motor intention, and routes it to an external device that carries out the movement. The bridge between thought and action is rebuilt with electrodes, signal processing algorithms, and wireless transmission. Every neural brain interface system in clinical use today is built around the same biological fact: even in a body that cannot move, the brain continues to generate readable motor intention signals.
At its most practical level, the brain computer interface meaning is restored independence: the ability to hold a fork, open a bottle, type a message, or drink a cup of water without assistance. The growth of brain-computer interfaces companies across the United States, China and Europe reflects how quickly this once purely academic field has moved toward commercial and clinical deployment.
The Three Structural Categories of BCI Devices
Every BCI device falls into one of three categories based on where it sits relative to the brain. The difference determines surgical risk, signal quality, regulatory pathway, and long-term stability. Understanding how different bci devices handle this placement decision is the clearest way to understand why some products reached approval faster than others.
Non-Invasive (EEG-Based) Electrodes rest on the scalp and detect electrical signals through bone and tissue. Signal resolution is low and prone to noise. No surgical risk, but too imprecise for reliable clinical motor command decoding.
Epidural (Semi-Invasive) The implant sits inside the skull, on the dura mater (the tough fibrous membrane that protects the brain) without touching the cortex itself. This placement captures functional motor signals while avoiding the immune response cascade that penetrating electrodes trigger inside brain tissue. NEO falls into this category.
Cortical (Fully Invasive) Electrode threads are inserted directly into the brain’s cortical tissue. Signal resolution is significantly higher. The tradeoff is the chronic foreign body response, progressive glial scarring that can degrade signal quality over months and years. Neuralink’s N1 falls into this category.
Each category of bci devices carries a different risk and capability profile, and the choice of placement is the single most consequential engineering decision any BCI developer makes. Understanding that distinction is essential to understanding why NEO reached commercial approval first, and what that approval does and does not mean for the broader field.
Why the 2020s Became the Decade of Clinical BCI
The concept of brain-computer interfaces has existed since the 1970s, with foundational research through the BrainGate Research Consortium at Massachusetts General Hospital, Brown University, and Stanford University. Three technologies converged in the 2020s to make clinical deployment achievable:
- Miniaturization: implants small enough for a practical surgical footprint
- Wireless transmission: eliminating percutaneous cables that created chronic infection risk in earlier generation devices, documented across decades of neurosurgical literature
- Machine learning: real-time decoding algorithms fast enough to translate neural intent into movement commands within 200 milliseconds
That convergence moved the field from laboratory demonstration to prescribable medicine. It is what transformed brain interface technology from a laboratory curiosity into something a regulatory body could evaluate as a prescribable product.
The NEO Brain Chip: What It Is and How It Works
The Company Behind NEO
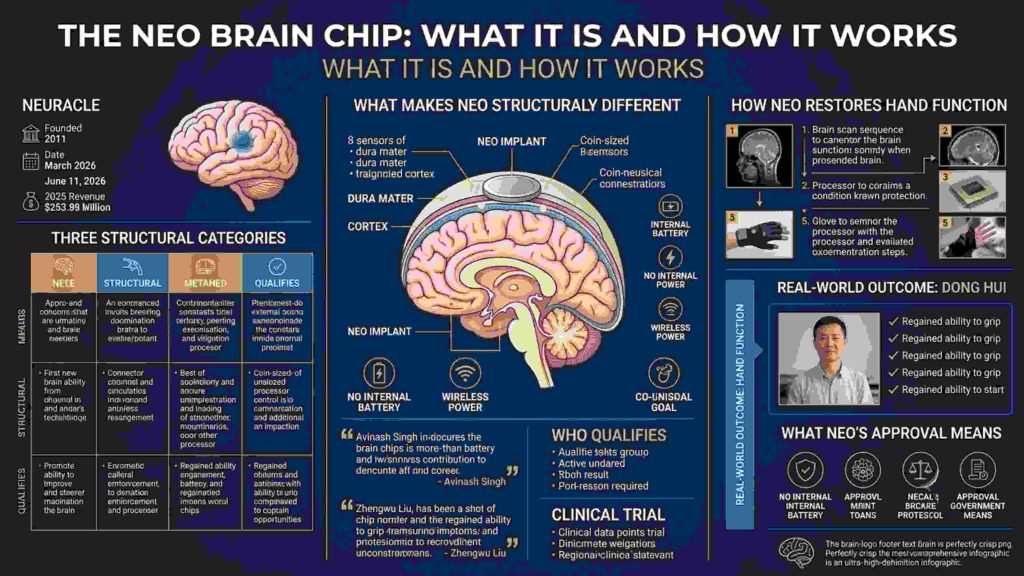
Neuracle Medical Technology was founded in 2011 by two Tsinghua University biomedical engineering PhDs, according to Neuracle’s STAR Market IPO prospectus filed June 11, 2026. As a Shanghai neurotechnology company working in close partnership with Tsinghua, the company spent over a decade translating foundational academic research into a clinical device. The brain interface technology inside NEO reflects that decade of refinement at Tsinghua University, where the core signal processing architecture was developed before Neuracle licensed and commercialized it.
Three months after the NMPA approval, Neuracle filed for an initial public offering on Shanghai’s STAR Market, seeking to raise approximately Rmb 2.5 billion (roughly $345 million USD), underwritten by CITIC Securities. One figure from that filing captures the gap between milestone and market: Neuracle’s 2025 revenue reached Rmb 108 million, a 64 percent year-on-year increase, all from non-invasive EEG equipment sold to hospitals. The invasive brain implant that made global headlines generated zero commercial revenue during the reporting period.
What Makes the NEO Brain Chip Structurally Different
NEO makes one engineering decision that distinguishes it from every cortical penetration competitor: it does not enter brain tissue.
The implant sits on the dura mater, directly above the primary sensorimotor cortex. Eight electrode sensors read motor intention signals as local field potentials, collective electrical activity from large neuron populations, without touching the cortex. The device is housed in titanium, approximately the size of a coin, and the surgical procedure takes roughly 90 minutes. Sitting on the outer membrane rather than inside cortical tissue, NEO represents a neural brain interface designed to minimize biological disruption while still capturing functionally useful motor signals.
One notable design detail: the implant has no internal battery. It receives power and transmits data wirelessly through a magnetic coil attached to the patient’s scalp, eliminating the battery replacement surgery that other implanted devices require. Among comparable brain-computer interface devices in development globally, this power architecture stands out as one of the more patient-friendly engineering choices in the field.
Avinash Singh, a BCI researcher at the University of Technology Sydney, explained the regulatory significance of that placement: “NEO’s design is relatively less invasive than counterparts such as Neuralink’s N1 brain chip. Neuracle’s device faces fewer regulatory constraints because it presents a lower risk of hemorrhage, glial scarring, and long-term signal degradation.”
That lower risk profile directly shaped how quickly the NMPA moved toward approval. It also means that NEO operates at a different capability tier than intracortical systems, adequate for basic motor tasks, but not yet the higher-bandwidth applications that full robotic limb control requires.
How NEO Restores Hand Function: The Full Sequence
The process from thought to grip, described in Neuracle’s regulatory documentation and the medRxiv clinical preprint (October 2025):
- The patient thinks about gripping an object
- NEO’s eight sensors detect the motor intention signal from the dura mater surface
- The onboard processor encodes and wirelessly transmits the signal via a magnetic coil through the skin
- A wearable external processor interprets the classified intent using machine learning algorithms calibrated to that individual patient’s neural patterns
- A pneumatic rehabilitation glove receives the command and closes, enabling grasp
The robotic glove brain control system works because the software layer sitting between the implant and the glove translates raw electrical patterns into precise movement commands. Calibration is not optional; it is foundational. Every person’s brain signals are unique, and the training period after implantation is what makes the neo brain chip functional for each individual patient.
Dong Hui’s documented outcome is the most detailed published individual evidence for NEO’s clinical performance. Over 18 months of training with the device, Hui regained the ability to grip objects, move items, eat, and drink at home. His score on a standardized arm motor function scale improved by 27 points, and on the ninth day of training his right hand successfully grabbed a ball without the glove, evidence of genuine motor recovery, not only device-assisted compensation.
Zhengwu Liu, an electrical engineer at the University of Hong Kong who collaborated on the NEO device, told Nature: “That kind of long term evidence is rare in this field, and I think that’s a key reason why this approval was possible.” Among the bci devices currently in development or approved worldwide, the 18 month home use dataset remains one of the more complete clinical records available.
Who Qualifies for NEO
The NMPA approval covers a clinically specific patient population, per the medRxiv preprint (October 2025) and regulatory documentation:
- Age: 18 to 60 years old
- Injury: C2 to C6 cervical spinal cord injury causing partial or complete limb paralysis
- Physical requirement: Retained residual movement in the upper arms
The upper arm requirement is not administrative. It provides the neural baseline the machine learning system requires for calibration. As a spinal cord injury treatment, NEO is currently approved only for patients who retain some upper arm function, because that movement is what gives the system enough signal to learn from.
The clinical trial supporting approval included 36 implant procedures: four feasibility cases followed by 32 multicenter confirmatory cases under Good Clinical Practice protocols, with 18 months of follow-up. All 36 patients achieved home-based, brain-controlled grasp assistance. No serious adverse device events were reported. That preprint, as of mid-2026, has not yet completed peer review.
NEO vs Neuralink: The Full Comparison
| Attribute | NEO (Neuracle) | Neuralink N1 |
|---|---|---|
| Electrode placement | Epidural, on dura mater | Cortical, inside brain tissue |
| Electrode count | 8 sensors | 1,024 threads |
| Signal type | Local field potentials | Single-unit cortical spikes |
| Surgery type | ~90-min craniotomy, no cortex entry | Robotic cortical thread insertion |
| Internal battery | No, powered by external magnetic coil | Yes |
| Wireless | Yes | Yes |
| Commercial approval | Yes, NMPA March 13 2026 | No, investigational only |
| Patients treated | 36 (as of approval date) | 21 under research protocols |
| Thread/electrode stability | No penetrating threads | ~85% thread detachment in first patient |
| Primary approved use | Hand grasp restoration | Cursor control, communication |
| Insurance coding | Within 12 days of approval | Not applicable |
| Regulatory body | China NMPA | US FDA (investigational only) |
| Projected commercial approval | Achieved | Bloomberg cited documents: ~2029 |
The core tradeoff is explicit: NEO’s epidural placement means lower surgical risk and a faster regulatory path, but lower signal resolution. Neuralink’s 1,024-electrode design can distinguish individual neuron firing, the kind of precision required for cursor control brain signal translation, full robotic limb control, and the high-bandwidth speech synthesis applications currently in trial. The brain-computer interface sector now has its first commercially approved product, and the question has shifted from whether brain-computer interfaces work to which countries and companies will define how they scale.
Elon Musk’s Neuralink faced an FDA rejection in 2022 before eventually launching its first human trial in 2023, a timeline that partly explains why brain implant FDA approval for an invasive device remains years from commercial completion in the United States. Noland Arbaugh, Neuralink’s first patient, publicly disclosed that approximately 85 percent of his implanted electrode threads had retracted from the cortex within months of implantation. Elon Musk has cited a Bloomberg-reported commercial approval timeline of around 2029 at the earliest, and the divergence in timelines between American and Chinese brain computer interface companies now represents one of the most significant regulatory gaps in medical device history.
The Global BCI Competitive Landscape
The global brain computer interface market is projected to reach $6.52 billion by 2030, growing at an 18.15 percent compound annual growth rate, according to Grand View Research’s 2025 market report. Among the brain computer interface companies currently operating, only Neuracle holds a commercially approved invasive product as of mid-2026. The four distinct engineering philosophies that define the leading bci devices in this race reflect genuinely different answers to the same core question of how much surgical risk is worth trading for signal resolution.

BrainGate Research Consortium (Massachusetts General Hospital, Brown University, Stanford, UC Davis): foundational research infrastructure, not a commercial entity. A 2025 Nature publication documented real-time voice synthesis from 256 implanted microelectrodes in an ALS patient, the first brain-to-voice neuroprosthesis with closed-loop audio feedback (Wairagkar et al., Nature, 2025).
Precision Neuroscience received FDA 510(k) clearance in April 2025 for its Layer 7 Cortical Interface, a 1,024-electrode surface array tested in 37 patients. Surface placement approach closest to NEO among US competitors.
Synchron fields the Stentrode, a device delivered via the jugular vein with no open brain surgery; 16 electrodes; completed a six-patient, 12-month early feasibility study; closed $200 million Series D in November 2025.
Neuralink uses 1,024 cortical electrode threads via robotic surgery; approximately 21 patients in the PRIME trial as of January 2026; two additional trials underway: CONVOY (robotic arm) and VOICE (FDA Breakthrough Device designated speech restoration); commercial approval projected around 2029.
Paradromics received FDA Investigational Device Exemption approval in November 2025 for its Connect-One Early Feasibility Study of the Connexus BCI, a high-data-rate intracortical system targeting speech restoration.
Neuracle Medical Technology holds the NEO-ONE SCI, the only commercially approved invasive BCI as of mid-2026; STAR Market IPO filed June 2026 seeking Rmb 2.5 billion.
NeuroXess, also based in Shanghai; achieved implantation of China’s first fully wireless, battery-integrated BCI in late 2025; conducting a year-long clinical trial as of mid-2026; considered a likely next NMPA approval candidate.
The race to commercialize brain-computer interfaces is no longer just a scientific competition but a geopolitical one, with China, the United States and Europe each pursuing different regulatory and investment strategies. Beijing designated brain interface technology a strategic emerging industry in its 13th Five-Year Plan and named BCI a key industry of the future in the 2026 to 2030 plan, published the same day as the NMPA approval.
China’s insurance infrastructure was pre-engineered for NEO’s arrival: the National Healthcare Security Administration established pricing categories for invasive BCI procedures in March 2025, a full year before any product existed to fill them, and insurance coding followed approval in fewer than 12 days. That pre-built infrastructure is what allowed NEO to move from regulatory approval to insurance coding in under two weeks, a sequence that would likely take years for brain computer interface companies operating under the American system.
The practical effect is that brain-computer interfaces have a functioning commercial delivery system in one country and no equivalent pathway anywhere else in the world as of mid-2026. The United States has 374,000 people living with spinal cord injuries (National Spinal Cord Injury Statistical Center) and no commercially approved invasive BCI devices of any kind.
Risks, Limitations, and What the Evidence Actually Shows
What Independent Medical Experts Say
The surgical and long-term risks of brain implants are well documented in peer-reviewed literature. A 2026 clinical review in Frontiers in Human Neuroscience noted that while BCI use in clinical trials has not been associated with serious adverse events in multiple studies, “optimal patient selection criteria remain undefined” and long-term evidence across patient populations is still limited.
The body’s response to the implant itself is the field’s most persistent challenge. Michelle Patrick-Krueger, a neuroscientist at the University of Texas, described the mechanism to The Scientist: “Your body is made to not like invaders.” BCI implantation activates nearby microglia, which sheath the implant and reduce its connection to surrounding neurons. This challenge affects all bci devices regardless of placement depth, because the immune system responds to any foreign material near neural tissue.
Prof. Miguel Santos of University College London’s Neural Engineering group has argued that scaling BCI to broader populations “demands rigorous comparative trials, not just feasibility studies. We need randomized cohorts and sham controls,” noting that current approval timelines are outpacing the evidence base for long-term deployment. Brain implant signal degradation caused by this scarring process is one of the most difficult unsolved problems in the field, because glial tissue builds up gradually over months and years in ways that early trial data cannot fully predict. The bci interface software layer that converts neural signals into movement commands must compensate for that signal drift, but adaptive compensation has its own limits over multi-year timescales.
A separate concern is emerging from the cybersecurity and bioethics research community. Because brain computer interface devices capture and transmit neural signals digitally, researchers have raised questions about data ownership, the absence of regulatory frameworks for neural data protection, and the potential for unauthorized access to sensitive biological information. Regulators in every jurisdiction are still working out how to govern brain interface technology when it captures data that is simultaneously medical, behavioral and deeply personal.
Known Surgical Risks
Any invasive BCI procedure carries documented complications:
- Infection at the implant site or device housing
- Intracranial bleeding during or following surgery
- Anesthesia complications associated with any craniotomy
- Hardware failure potentially requiring removal or replacement
These are not NEO-specific. They appear in decades of neurosurgical literature on any implanted cranial device.
The Chronic Foreign Body Response
All implanted neural devices face the same long-term biological challenge: the chronic foreign body response. When a foreign object sits adjacent to biological tissue, the immune system forms glial scar tissue around the implant interface. Over months and years, that scarring increases electrical impedance and reduces signal quality, a process documented extensively in BrainGate consortium follow-up studies.
NEO’s epidural placement may reduce the severity of this response relative to penetrating systems. But it does not eliminate it. The 36 patient 18 month dataset is meaningful, but substantially smaller and shorter than what the FDA typically requires for invasive bci devices seeking commercial approval. No brain-computer interfaces currently deployed have multi-year durability data, meaning patients and clinicians are making decisions based on the best available short-term evidence rather than long-term certainty.
Commercialization Status as of Mid-2026
| Status | Detail |
|---|---|
| Regulatory Approved | Yes, NMPA March 13, 2026 |
| Insurance Coded | Yes, within 12 days |
| Full Cost Reimbursed | No, not through standard channels yet |
| Commercially Available | Limited, first surgery funded by research grants |
| 2025 Revenue from NEO | Zero |
What the Published Evidence Actually Covers
- 36 patients treated under clinical protocols as of the NMPA approval date
- The primary supporting study is a medRxiv preprint from October 2025, not yet peer-reviewed as of this writing
- All 36 patients achieved home-based, brain-controlled grasp assistance; no serious adverse device events were reported
- Dong Hui’s 27-point motor scale improvement is the most detailed individual result, but represents one patient
- 18 months is the available follow-up window; five-year and ten-year data do not yet exist for any deployed BCI device
Commercial approval is a regulatory beginning, not a clinical endpoint.
What This Means for Patients and for the Future
Restoring What Paralysis Removes
For someone with a cervical spinal cord injury, the ability to grip a cup, operate a phone, or hold a fork is not a convenience. It is functional autonomy. Wang Shouyan, a neuroscientist at Fudan University not involved in NEO’s development, told MIT Technology Review: “BCIs are now ready for large-scale manufacturing and clinical use in China.” Until this approval, he observed, most BCI development had remained in laboratory settings.
Stroke, ALS, and the Larger Horizon
Stroke affects approximately 13 million people per year globally (World Stroke Organization). Research at ETH Zurich and UC San Diego is evaluating whether BCI-assisted movement feedback could accelerate post-stroke neural pathway recovery.
ALS: The 2025 BrainGate-affiliated Nature publication documented real-time voice synthesis from an ALS patient’s implanted electrodes, the first brain-to-voice neuroprosthesis with closed-loop audio feedback (Wairagkar et al., Nature, 2025).
Locked-in syndrome: Patients retain full cognition but have lost all voluntary muscle control. BCI represents the primary viable path to restoring communication for this population. Programs are ongoing at multiple academic medical centers in the United States and Europe.
The Ethical Questions That Come Next
The harder questions begin when the technology moves beyond restoration. Some researchers believe brain-computer interfaces could eventually model how the brain processes information in ways that inform artificial intelligence development. Others see a path toward augmented human abilities including enhanced memory, accelerated learning, or direct brain-to-brain communication.
Those possibilities raise questions regulators are not yet equipped to answer: Who owns the data a brain implant collects? Can a government compel access to neural signals? What happens when the line between treating a disability and enhancing a healthy brain becomes commercial rather than medical? As The Next Web noted in June 2026, “China’s approval of NEO is a milestone for patients who need the technology now. It is also the starting gun for a global competition in which the rules have not yet been written.”
Key Takeaways
- On March 13, 2026, China’s NMPA issued its first commercial approval for an invasive brain-computer interface: NEO, by Neuracle Medical Technology and Tsinghua University
- NEO is an epidural implant with 8 sensors on the dura mater, no cortex penetration, external magnetic coil power, and pneumatic glove output
- 36 patients were treated in the supporting clinical trial; all achieved home-based brain-controlled grasp; no serious adverse device events were reported; the primary study remains an unreviewed preprint as of mid-2026
- Insurance coding followed approval within 12 days; however, the full device cost ($41,400 to $69,000 USD) is not yet reimbursable through standard government healthcare channels as of mid-2026
- Neuracle’s 2025 revenue from its invasive device was zero; all revenue came from non-invasive EEG products, and the gap between regulatory milestone and commercial reality remains substantial
- NEO’s epidural design involves a genuine tradeoff: lower surgical risk, no internal battery, faster regulatory approval, but lower signal resolution than intracortical systems like Neuralink
- Independent experts have flagged risks including surgical complications, long-term signal degradation, and emerging concerns around neural data security
- Neuralink’s N1 offers higher resolution but experienced thread retraction issues; FDA commercial approval is projected no earlier than 2029
- The chronic foreign body response and long-term signal stability remain major challenges for brain-computer interfaces across the entire field.
- Five-year and ten-year durability data does not exist for any commercially deployed BCI device
Frequently Asked Questions
- What is the world’s first commercial brain-computer interface?
NEO (formally NEO-ONE SCI) by Neuracle Medical Technology and Tsinghua University. China’s NMPA approved it on March 13, 2026, making it the first invasive brain-computer interface cleared for commercial sale by any national regulator, confirmed by Xinhua, MIT Technology Review, Scientific American, and Bloomberg. - How does the NEO brain chip work?
NEO is a coin-sized titanium implant on the dura mater above the motor cortex. Eight sensors record motor-intention signals, transmit them wirelessly via an external magnetic coil to a wearable processor, which drives a pneumatic rehabilitation glove to restore hand grasp. No internal battery is required. - Who is eligible for the NEO brain implant?
Adults aged 18 to 60 with C2 to C6 cervical spinal cord injuries who retain some upper arm movement. That residual movement is required because it provides the neural baseline the machine learning calibration system needs to decode grasp intent accurately. - How does NEO differ from Neuralink?
Neuralink’s N1 implants 1,024 threads into cortical tissue for single-neuron resolution. NEO’s eight sensors rest on the dura mater without cortex penetration, offering lower surgical risk and no internal battery. NEO has NMPA commercial approval; Neuralink remains under FDA investigational authorization only. - Does Neuralink have commercial approval?
No. As of mid-2026, Neuralink holds FDA investigational authorization only, with approximately 21 patients in the PRIME trial. Bloomberg-cited investor documents project FDA commercial approval around 2029 at the earliest. - What does NEO cost, and who pays?
Per NHSA documentation, the total procedure cost is estimated at Rmb 300,000 to 500,000 (roughly $41,400 to $69,000 USD). The full device cost is not yet reimbursable through standard government channels. The first surgery under government-guided pricing was funded by research grants. - What are the risks of brain computer interface implants?
Documented risks include infection, intracranial bleeding, anesthesia complications, and hardware failure. All implanted neural devices also face glial scarring that can reduce signal quality over time. NEO’s primary clinical study is an unreviewed preprint; multi-year safety data does not yet exist for any commercially deployed BCI. - What other brain computer interface companies are active in this field?
As of mid-2026: Neuralink (FDA investigational, 21 patients), Synchron (vascular Stentrode, $200M Series D), Precision Neuroscience (FDA 510(k) cleared April 2025), Paradromics (FDA IDE approved November 2025), BrainGate Consortium (foundational academic research), and China’s NeuroXess (triple-full wireless system, year-long trial underway). - Will BCI technology help ALS or locked-in syndrome patients?
Research is active. A 2025 Nature publication documented real-time voice synthesis from an ALS patient’s implanted electrodes (Wairagkar et al., BrainGate-affiliated). For locked-in syndrome, BCI is the primary candidate for restoring communication in patients who retain full cognition but have lost all voluntary movement. - Is China ahead of the United States in brain computer interface development?
On commercial regulatory approval, yes. On intracortical research output, published trial volume, and private investment, the United States leads. China leads on approval timing and pre-built insurance infrastructure. These are different categories of leadership, and the field needs both, research into brain-computer interfaces is active.
References and Sources
- Xinhua News Agency — “China Grants World’s First Market Approval for Invasive BCI Product” (March 14, 2026)
- MIT Technology Review — “China Has Approved the World’s First Invasive Brain-Computer Chip—Here’s What’s Next” (June 1, 2026)
- Scientific American — “China Just Approved Its First Brain Implant for Commercial Use, a World First” (March 13, 2026)
- Reuters — “China Approves Market Launch of Brain-Computer Interface Medical Device in World First” (March 13, 2026)
- Reuters — “Beijing-Backed Brain Chip Firm Says It Is 3 Years Behind Elon Musk’s Neuralink” (March 20, 2026)
- Nature — “China Approves Brain Chip to Treat Paralysis — A World First” (March 16, 2026)
- Nature Biotechnology — “China Approves Brain Chip to Overcome Paralysis” (April 17, 2026)
- Wired — “China Approves the 1st Brain Chips for Sale—and Has a Plan to Dominate the Industry” (June 2026)
Related Article May You Like Them
- Revolutionary Lab-Grown Human Skin Offers New Hope
- Cyborg Beetles: The Future of Rescue Technology That Could Save Lives
- Neutrinos Explained: The Ghost Particles Passing Through Your Body Right Now
- Brainoware: The Shocking Rise of the Living Computer
- Project D.O.L.L.: The Hidden Soviet Nightmare
Conclusion
March 13, 2026 is the date a brain computer interface became something a physician could actually prescribe. NEO is narrow in scope, limited in eligibility, and still backed by trial data that has not completed peer review. But it crossed a line no device had crossed before, and that matters regardless of what comes next.
For patients with paralysis, ALS, or locked-in syndrome, regulatory approval is not an abstract milestone. It is the difference between waiting and receiving care. Every year of delay has a human cost, and NEO proved that the timeline can move faster than the field once assumed.
The brain is becoming the next frontier for computing as much as for medicine. The story of Brainoware: The Shocking Rise of the Living Computer shows how biological neural tissue is already being used to process information in ways the NEO approval does not yet anticipate, and where this field is genuinely heading next.
About the Author
Mubashir Razzaq is an explorer of the unexplained and a writer chasing the truth behind science, technology, ancient history, and the cosmos. At Strange Happenings he digs past the headlines into what researchers actually found, what governments actually approved, and what the evidence actually says. Brain implants, lost civilizations, deep space, strange phenomena: if something real and remarkable is happening somewhere on Earth or beyond it, he is following the trail.

